Overview of surgical techniques
The surgical strategy depends on the tumour type, location, extent and the patient's overall condition. The spectrum ranges from targeted, minimally invasive procedures to multi-hour, multi-specialty complex resections.
En bloc resection
Removal of the tumour in a single piece with intact surgical margins — the international standard for the radical treatment of primary malignant spine tumours. This technique maximises the chance of local control and provides the best long-term oncological outcome. A technically and time-demanding operation that requires precise preoperative planning.
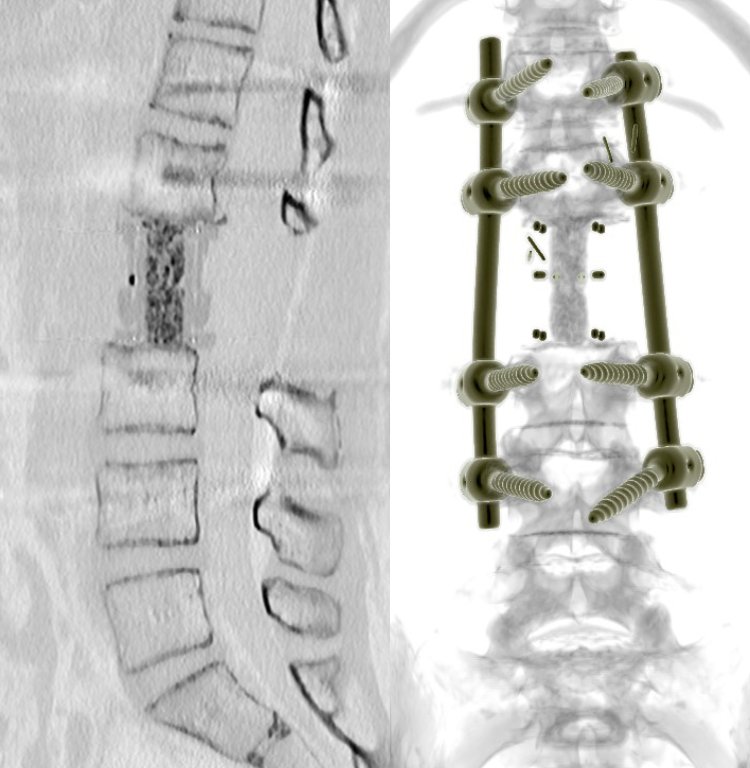
Complex reconstructive surgery
Restoration of spinal stability after tumour removal, using a tumour prosthesis, titanium implants, cages and bone-graft substitute. For sacral and larger resections, the involvement of abdominal and plastic surgeons is also required for closure and reconstruction.
Minimally invasive procedures
For spinal metastases, where the goal is rapid pain control and preservation of neurological function: percutaneous stabilization, vertebroplasty (cement injection into the vertebra), and in selected cases radiofrequency ablation. These procedures involve a short hospital stay and faster recovery.
Urgent nerve decompression
In a patient with cancer, sudden new neurological symptoms — limb weakness, gait disturbance, pathological vertebral fracture — represent an urgent surgical indication. Rapid nerve decompression is critical for preserving function, often before oncological treatment begins.
