Anatomical background
What is disc herniation?
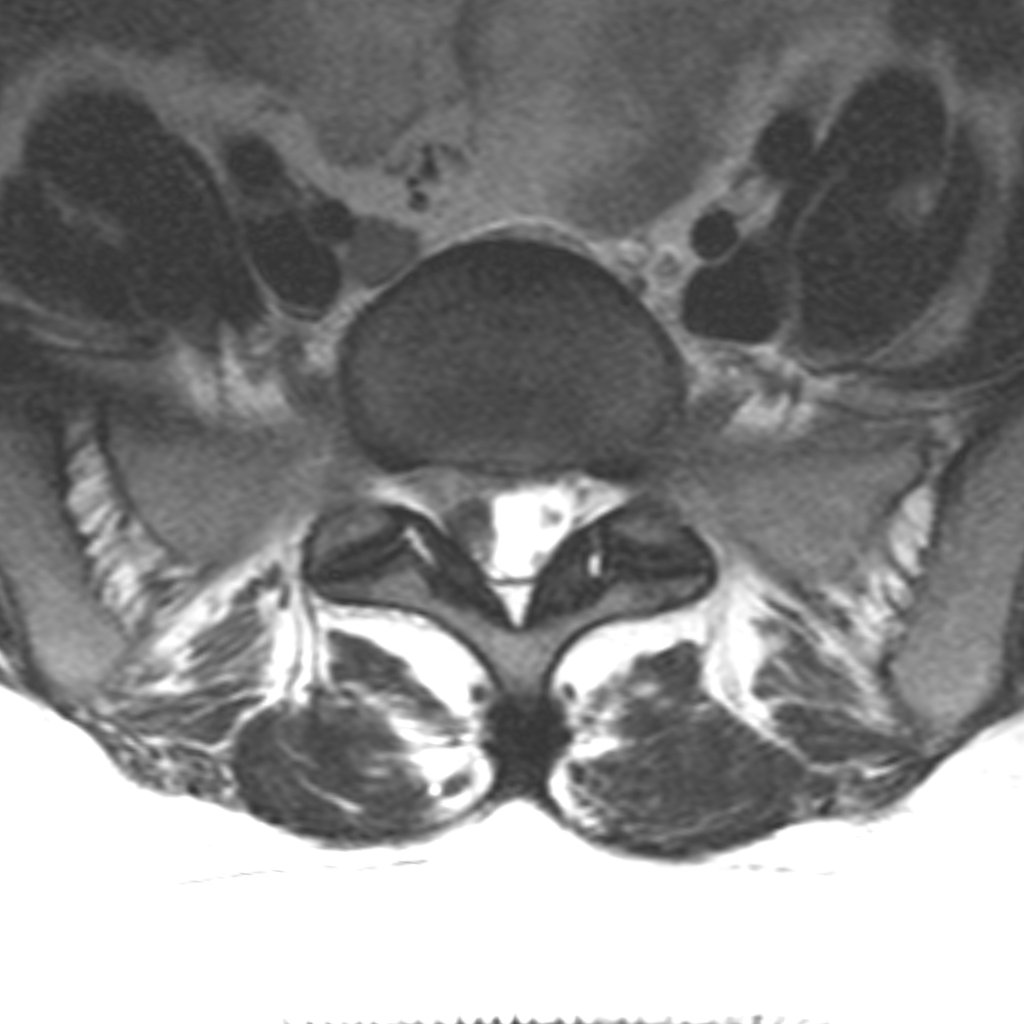
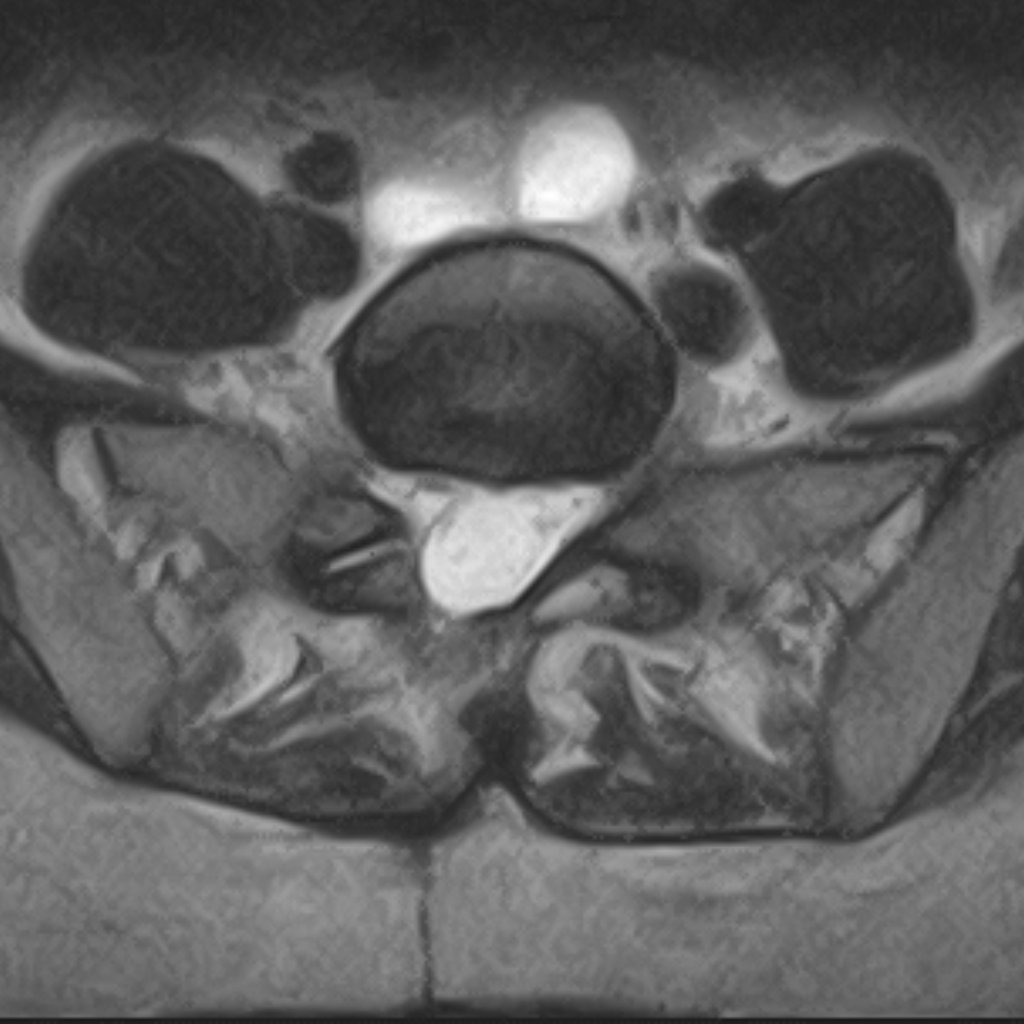
The intervertebral discs between the vertebrae act as flexible cushions that absorb load and allow movement. The fibrous outer wall of the disc (annulus fibrosus) can weaken over time, and a bulge can form on it, putting pressure on the nerves running directly alongside.
Another presentation is the sequestrated disc herniation: a tear forms in the fibrous ring, through which the gel-like material from inside the disc (nucleus pulposus) escapes outside the disc. In this case, in addition to the mechanical pressure on the nerve, the chemical properties of the displaced material also irritate the nerves. Pressure and chemical irritation together create inflammation in the neural elements, which sustains the pain syndrome.